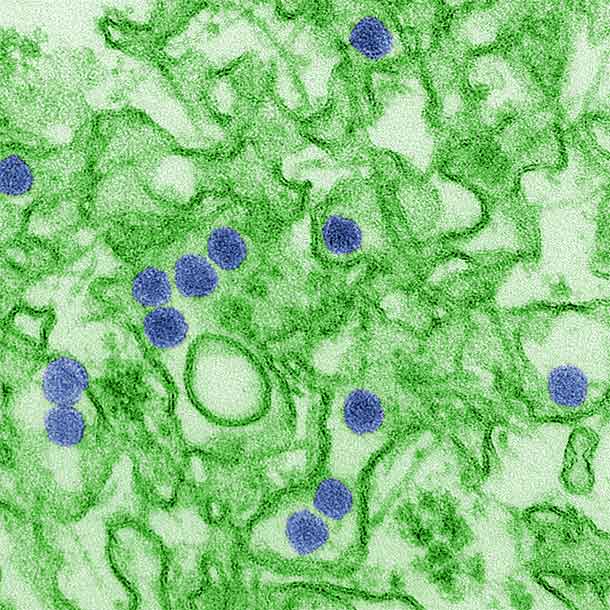
In 1947, the mosquito-borne Zika virus (ZIKV) was first isolated from a rhesus monkey in the Zika forest of Uganda. In 1968, isolation from human hosts occurred in residents of Nigeria. Multiple studies have confirmed ZIKV antibody in humans from a multitude of countries in Africa and parts of Asia. In 2015, ZIKV first appeared outside of Africa and Asia when it was isolated in Brazil.
ZIKV is closely related to other mosquito-borne flaviviruses such as the dengue, Japanese encephalitis, yellow fever, West Nile viruses. ZIKV causes a disease known as Zika fever, which is characterized by a macropapular rash covering the body, fever, joint pain, and malaise. ZIKV is an important emerging pathogen due to its appearance across the globe, mosquito-driven transmission cycle, and possible spread via sexual contact. Studies have shown that ZIKV can reside in blood transfusions and they can be a possible vector for human-to-human transmission.
Diagnosis for ZIKV infection include PCR tests to detect viral DNA as well as additional tests to detect ZIKV antibody (IgM) in serum. IgM for ZIKV is typically detectable around 3-5 days after infection, but cross-reactivity with closely related dengue, yellow fever, Japanese encephalitis, and West Nile viruses are possible.
There is no vaccine for ZIKV or treatment for Zika fever. Symptoms are relatively mild and only supportive therapy is employed.
We accept the following payment methods as well as pay-by-invoice.